
Whole Picture Public Health Approach Datasets 2021-24 Professional Survey
This data is from a survey completed by professionals who were involved in the SafeLives Public Health Approach between 01/07/2021 and 22/09/2024.
Welcome to our brand new website, providing you with easier access to our training, research and resources!
At SafeLives, our mission is to end domestic abuse, for everyone and for good. We take a holistic, public health approach to ending domestic abuse.
To end domestic abuse, we need to look at the whole picture.
This means:
Our team of practice experts supports local areas with systemic change, developing an understanding of local organisational culture, context and connections, mobilising the ambitions within our own strategy and local plans, to end domestic abuse.
We work with local authorities, Police and Crime Commissioners, Clinical Commissioning groups and other multi-agency partners to undertake a systemic review through the lens of the whole family, identifying opportunities for improving the response to high risk abuse, as well as early intervention and prevention. Our approach includes a systems-wide assessment of the current local landscape, consulting with service users and providers to understand opportunities, strengths, and gaps.
We co-create solutions through delivery of workshops based on the understanding of the system and make recommendations for improvement, enhancing existing work and – in England and Wales – supporting areas implement the new requirements of the Domestic Abuse Act 2021.
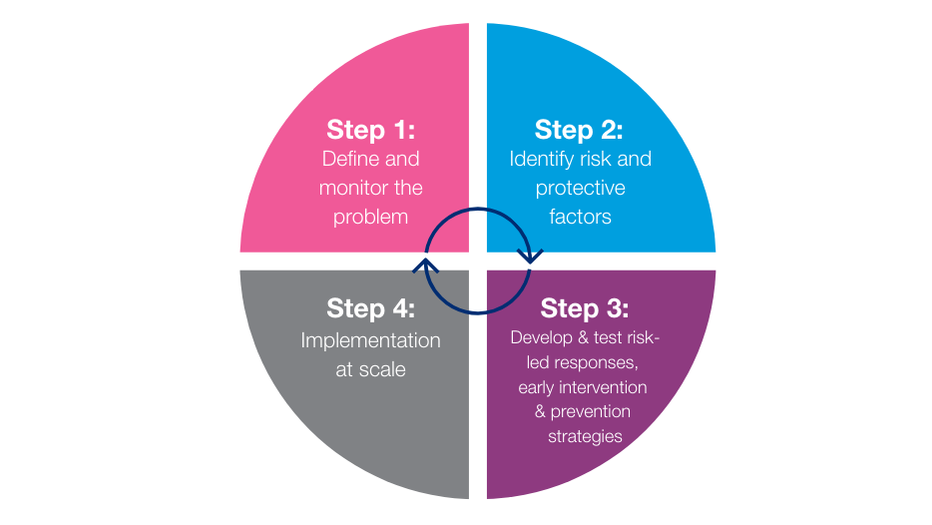
To date, SafeLives has worked with 27 Local Authorities in England and Wales on the first two steps. We’re proud to publish our Executive Summary report which shares the findings of this work to date. These findings are based on extensive research which includes surveys and interviews with survivors, professionals and those who harm. The report tells us:
Read the Report and Executive Summary
The practice team in SafeLives bring together a wealth of domestic abuse and multi-agency experience including housing, health, social care, safeguarding and youth work. We use our knowledge, experience, and research capabilities to support and advise areas in developing a whole family, systems wide approach in preventing and responding to domestic abuse. Key to the success of our work is embedding the voice of survivors and taking an evidenced based approach. We build what we do in areas by understanding in depth what is happening, through both qualitative and quantitative data; identifying opportunities and strengths; then co-creating with key stakeholders’ solutions which are based on what works.
To discuss how we can support your area, please contact our Head of Practice.
Survivor of domestic abuse“We must talk about it more - in the media, in places of work, normalise it without accepting it and helping people have the courage on the outside to challenge it. If we can fundamentally change attitudes around drink driving and smoking - surely we can start to raise awareness and address domestic abuse in the same way. If survivors, children and young people get behind this - we can change the future.”
Our research, data, interventions and survivor feedback, has shown how local systems fail to understand the whole picture of a family affected by domestic abuse.
Survivor of domestic abuse“All professionals need to be informed about how to work with those affected by domestic abuse, and the perpetrators. It is not a specialist area of work – it is the bread and butter for everyone who works with families in all capacities. It is not a standalone issue – people need to understand how it relates to all other areas of people’s lives in complex ways.”


Sign up to receive our monthly newsletters about the latest training, events, research and fundraising initiatives at SafeLives. Together, we can end domestic abuse, for everyone, for good.