A Cry for Health
Why we must invest in domestic abuse services in hospitals.
Welcome to our brand new website, providing you with easier access to our training, research and resources!

Research and resources for healthcare professionals providing care to victims of domestic abuse.
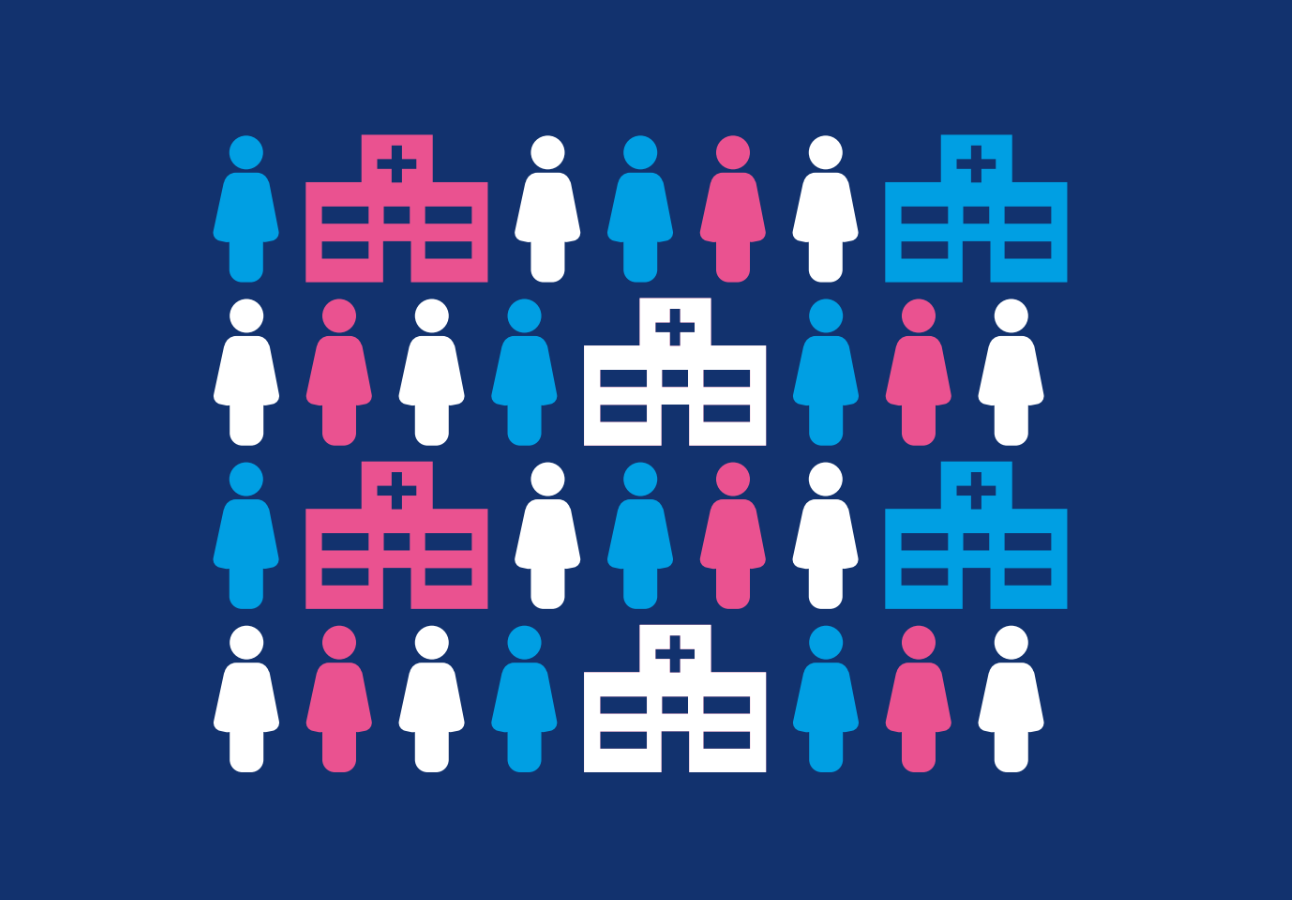
4 in 5 victims don’t go to the police, but almost all will visit a health service at one time or another. Asking about domestic abuse and giving the appropriate response must be routine if we are to identify all victims – particularly the most vulnerable.
By failing to ask a victim questions in hospital, we are enabling them to be discharged back into the arms of the perpetrator who put them there. We know risk increases in pregnancy, and that abuse is inextricably linked with mental health needs. Our research shows that experiencing domestic abuse is also an issue for staff working across healthcare systems.
We want to see a comprehensive health response across the UK, with Idvas co-located in hospital and all staff trained to ask, respond and refer.
and this may be their first or only contact with professionals.



(with mental health costs estimated at an additional £176 million)



Diana Barran, SafeLives founderDomestic abuse is a public health epidemic and health must be part of the solution. We must meet victims where they are. We know four of five victims do not call the police. We have to go to them: where they feel supported, where they feel safe and free from stigma.



SurvivorWhen I went to A+E the doctor told me we only do bones here, not that ‘relationship mental health stuff’. But didn’t offer to refer me to somewhere that did.
Tools and services for frontline domestic abuse professionals and services
Blogs from SafeLives staff, Pioneers and expert guests



Sign up to receive our monthly newsletters about the latest training, events, research and fundraising initiatives at SafeLives. Together, we can end domestic abuse, for everyone, for good.